








Background: Leprosy is a neglected disease caused by Mycobacterium leprae. Brazil has the second largest number of cases in the world.
Objectives: To analyze the spatial distribution of leprosy in the state of BAHIA, Brazil, and the association between his occurrence and the synthetic indicators of municipal socioeconomic performance, social vulnerability and income inequality.
Methods: An ecological study with secondary data obtained from the National System of Notifiable Diseases. Dependent variables: coefficient of detection in the general population and in the population under 15 years old and the rate of grade II of physical disability. Independent variables: Synthetic indicators of socioeconomic performance, social vulnerability and income inequality.
Results: The highest coefficients of detection of new cases in the general population and in children under 15 years old are concentrated in the north-west axis and in the southern region of the state. On the other hand, the highest rates of degree II of physical incapacity are concentrated in the north, northeast and south regions. Only the Index of Social and Economic Performance(IPESE)-Economy and Finance composed the final regression model of the general detection coefficients and in children under 15 years old. The municipalities with the highest indexes had the highest detection coefficients, reflecting the capacity to diagnose new cases.
Study Limitations: The use of synthetic indicators is a limitation of the study.
Conclusions: Leprosy presents a heterogeneous spatial pattern in the state of BAHIA, and the LPESE-Economics and Finance indicator is the only one with explanatory potential of the disease.
Hansen’s disease is a chronic and granulomatous neglected tropical disease caused by Mycobacterium Leprae or Hansen bacillus. It is a bacillus with high infectivity that attacks cutaneous and peripheral nerve cells, leading to dermato-neurological lesions that can range from a single lesion with decreased sensation to systemic involvement and permanent physical disabilities, besides psychosocial distress.1-4
Since the introduction of polychemotherapy in the 1980s, there was a marked reduction in the burden of Hansen’s disease worldwide, reaching the elimination level in 2000 as a worldwide health issue, although 15 nations were not able to achieve that then. Only in 2014, 213,899 new cases of the disease were registered throughout the world, being 18,869 (8.8%) of them in the child population.5 Ninety-four percent of cases were concentrated in 13 nations of the globe, with the first positions occupied by India and Brazil, respectively. India has the largest number of Hansen’s disease cases but Brazil occupies the first position in prevalence, being the only one that did not achieve the target of elimination of the disease as a public health issue.5
In Brazil, the distribution of Hansen’s disease is very heterogeneous. While some States have very low coefficients of detection, such as Rio Grande do Sul and Santa Catarina – with coefficients of 1.08 and 2.51/100.000 inhabitants in 2015, respectively – others, such as Mato Grosso, had a coefficient higher than 90 new cases per 100.000 inhabitants for the same year.6
Considering the absolute numbers of new diagnoses, the northeastern region occupied the first position in 2015, with 12,848 cases, corresponding to 44.7% of all patients notified all over the country. The distribution of Hansen’s disease is not homogeneous in the region either. While Rio Grande do Norte registered a coefficient of 7.81/100.000 inhabitants, in the State of Maranhão the coefficient reached 51.27/100.000. The State of Bahia occupies an intermediate position in the ranking of Hansen’s disease burden in Brazil. In 2015, the State occupied the 11th national position and the 5th among the northeastern States, with a global detection coefficient of 16.76/100.000, above the national mean for the same period (14.07/100.000).6
The search for explanations regarding the factors that act as determinants for the occurrence of Hansen’s disease has been notably important to understand this heterogeneous spatial distribution. Many studies have tried to establish relationships between the disease and socioeconomic factors, based on different units of analysis such as census sectors and municipalities. However, few have examined the synthetic indicators of the existing socioeconomic performance regarding its ability in explaining the dynamics of the disease.7-9
It is assumed that this relationship is not just linear as cause-effect. There is a complex network of inter-relationships between socioeconomic factors and the occurrence of Hansen’s disease. It is at this point that the spatial modeling of data and the combination of different mathematical models can help understand the phenomenon. Recently, these models have been in the spotlight of the health sector, for both diseases and injuries to human health.10-14
In view of what was discussed, the objective of this study was to analyze the spatial distribution of Hansen’s disease in the State of Bahia and the association between its occurrence and the synthetic indicators of municipal socioeconomic performance, of social vulnerability and income inequalities.
MethodsIt is an ecological study in the territory of the State of Bahia, located in the northeastern region of Brazil, consisting of 417 municipalities. The period of the study comprehended an interval of 15 years (2001 to 2015).
Three indicators of monitoring of the elimination process of Hansen’s disease as a public health problem (dependent variables) were analyzed, as stated in the decree 149/2016, that “approves all guidelines for the vigilance, attention and elimination of Hansen’s disease as a public health problem, with the aim of guiding health service managers and professionals”. They are: i) annual coefficient of detection of new cases of Hansen’s disease in the general population per 100.000 inhabitants; ii) annual coefficient of detection of new cases of Hansen’s disease in younger than 15 years of age per 100.000 inhabitants; iii) coefficient of new cases of Hansen’s disease with grade II of physical disability at the time of diagnosis per 100.000 inhabitants.
For the analysis, we adopted the classification as described in the above-mentioned legislation. Since the coefficient of grade II does not have established evaluation parameters, we adopted the same detection coefficient as in younger than 15 years of age.15
To calculate the indicators, we collected data from new diagnosed cases according to the municipality of residence, extracted from the Sistema Nacional de Agravos de Notificação (SINAN). Cases closed as diagnostic error, recurrences and duplicate files were excluded. The populational data needed to calculate the indicators were obtained from the Instituto Brasileiro de Geografia e Estatística (IBGE), 2010 census and inter-census predictions.
The study was divided into two stages, the first being destined to spatial analysis of Hansen’s disease in the State and the second destined to the association between the disease and the synthetic indicators of municipal performance.
In the first stage, the mean coefficients for the period (20012015) were calculated. The empiric local Bayesian model was used to soften the indicators with the aim of minimizing the random fluctuation of data from smaller areas and, therefore, providing more stability for the indicators.16-19 Of note, in 2010, according to census’ data, only 16 (3.8%) municipalities in Bahia had a population larger than 100.000 inhabitants. Besides this argument for the use of Bayesian model, there is also the problem of under-notification of the cases of the disease, resulting in a reduced number of events per municipality. The low number of cases leads to little representative and even distorted estimates of reality. In these cases, the Bayesian model is an important solution to obtain more accurate data.17,19
The objective of the model is to identify the distribution after the event (quantities not observed of a certain phenomenon) from the application of Bayes theorem, involving sampling data (likelihood function) and a group of observed data (distribution before the event).20-21 In the health sector, many authors have successfully used the softening method before applying the statistics of Moran.11,14,22-24
Subsequently, we tried to identify the existence of spatial dependency and autocorrelation of the epidemiological indicators using the global Moran’s index (MI) and the pseudo significance test. The local autocorrelation (Local Index of Spatial Association – LISA) was evaluated through the local Moran’s index. The scatter plot for Moran’s I was generated from the local MI to identify critical or transition areas, through which we compare the value of each municipality to the neighboring municipalities. The generated quadrants were interpreted as: Q1-High/high (positive values and positive means); Q2-Low/low (negative values and negative means); Q3-High/low (positive values and negative means); and Q4-Low/high (negative values and positive means). Based on the results obtained from the scatter plot for Moran’s I and the LISA, the theme maps LISA Map and Moran Map were created. LISA Map comes from the local Moran’s index to identify different patterns of statistical significance. Moran Map is similar to LISA Map but only considers the areas whose Moran indexes were significant (p<0.05). These areas are presented according to their location in the scatter plot of Moran’s I (Q1, Q2, Q3 and Q4).21,25
In the second stage, the independent variables were defined: index of municipal human development (IMHD) and its dimensions (longevity, education and income) and the Gini and Theil-L indexes (income inequality) obtained from the 2010 census (IBGE); index of social vulnerability (ISV) and its dimensions (urban infrastructure, human capital and income and work), obtained from the Atlas of Social Vulnerability, Instituto de Pesquisas Econômicas Aplicadas (IPEA); FIRJAN index of municipal development (FIMD) and its dimensions (education, health and employment and income) obtained from the database of the Federação das Indústrias do estado do Rio de Janeiro (FIR-JAN); and the socioeconomic performance index (IPESE) and its dimensions (education, health and economy and finances), obtained from the Superintendência de Estudos Econômicos e Sociais do Estado da Bahia (SEI-BA). All were based in the year of 2010.
Initially, we tried to identify the statistical correlation between the epidemiological indicators and the socioeconomic indicators using the bivariate analysis of Pearson (significance of 5%). We opted to convert the indicators into logarithmic rates in order to guarantee data normality. Afterwards, the independent variables were submitted to the multivariate regression analysis (Ordinary Least Squares-OLS) with the aim of verifying the variables most associated to the outcome, as suggested by Anselin.26 To compose this model, independent variables with a significant correlation with the dependent variables were selected. We also verified the multicollinearity criterion among the variables from the observation of tolerance and the variance inflation factor.
The necessity of incorporation to spatial effects was evaluated next, analyzing the residue independence through Moran’s index. Once the autocorrelation of residues was determined, the choice of the best model to be adopted took place with the application of Lagrange multiplier tests, as the decisive model proposed by Anselin et al.27 Two models are possible: Spatial Error Model and Spatial Lag Model. While the first considers spatial effects as inconveniences that should be removed, the second attributes to the variable response Y the ignored spatial autocorrelation. After the application of the model, we adopted the Akaike criteria (AIC) and Bayesian criteria of Schwarz (BIC), being the best model the one that shows the lowest values, and the likelihood log and coefficient of determination (R2), the best model being that with the higher values. We applied Moran’s statistics to the residues of spatial models with the aim of quantitatively identifying if the spatial autocorrelation was eliminated.
ANOVA statistics was applied to compare epidemiological indicators among the layers of the socioeconomic indicators that composed the final regression model. We adopted the Tamhane T2 post hoc and significance of 5%.
For the analyses, the software Terra View 4.2.2, provided by the Instituto Nacional de Pesquisas Espaciais (INPE); QGis 2.14.11, provided by Open Source Geospatial Foundation (OSGeo); GeoDa 1.8.10, provided by Center for Spatial Data Science – University of Chicago; and SPSS 22.0, provided by IBM Corporation were used. The territorial charts needed to create the maps were sourced from IBGE.
The study was approved by the committee of ethics in research of the Universidade Federal de Alagoas CAAE n. 70943617.5.0000.5013 and approval report n. 2.212.723/2017.
ResultsBetween 2001 and 2015, based on SINAN’s data, 42,227 new cases of Hansen’s disease were notified in the State of Bahia, with a mean of 2,815.1 cases/year. Of the total, 8.1% (n=3,430) of the patients were younger than 15 years, with a mean of 228.7 cases/year. Grade II of physical disability at diagnosis was present in 4.8% (n=2,032) of the individuals diagnosed.
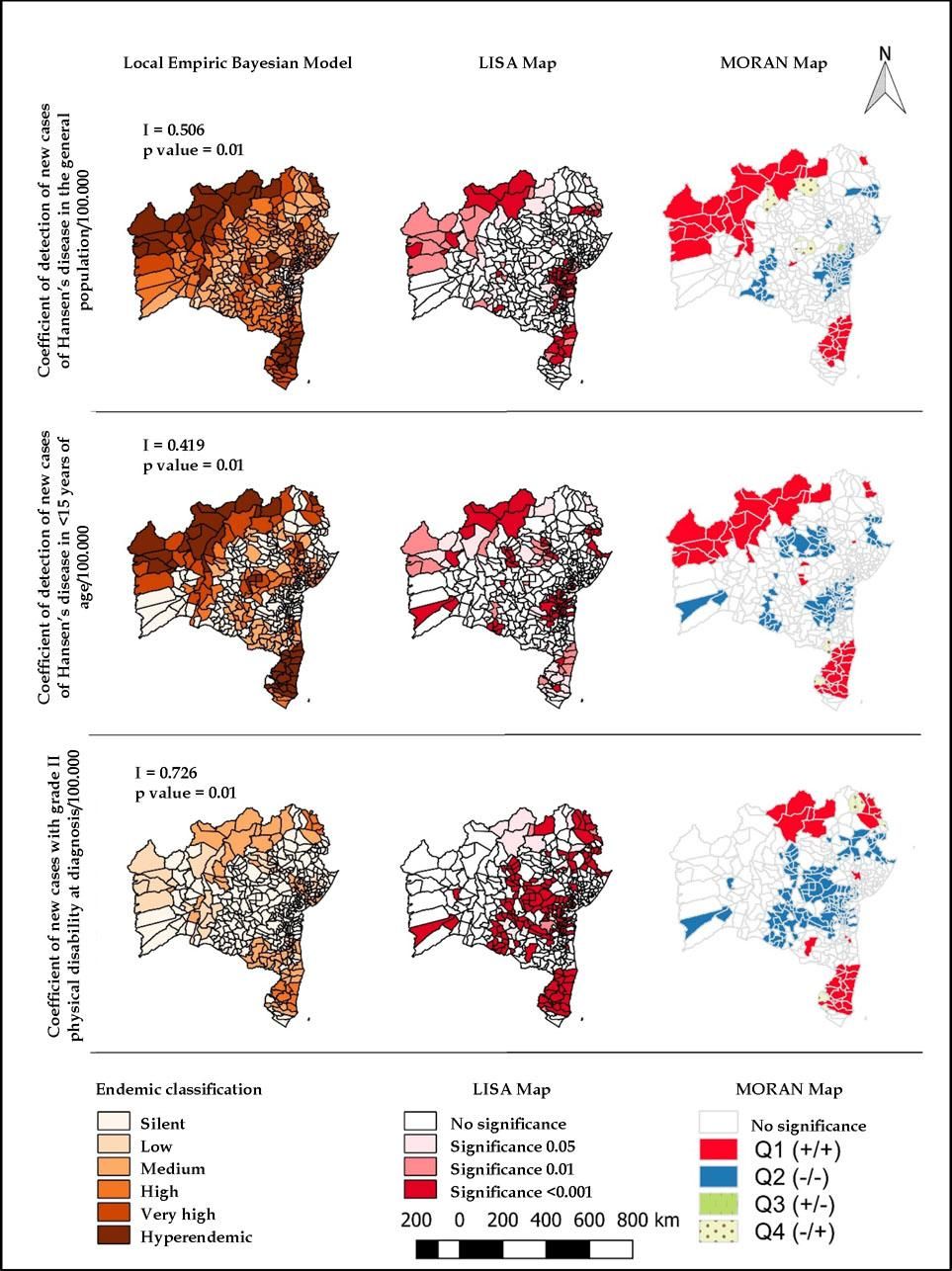
The spatial distribution of the disease in the State is not homogeneous (Figure 1). Global Moran’s index (I) showed that the three indicators had spatial autocorrelation: i) coefficient of general detection, I=506071 (p=0.01); ii) coefficient of detection in younger than 15 years, I=0,41992 (p=0.01); and iii) coefficient of physical disability grade II, I=0,726589 (p=0.01).
Spatial distribution of the coefficients of detection of new cases of Hansen’s disease in the general population and in younger than 15 years of age and the coefficient of new cases with grade II physical disability softened by the empiric local Bayesian model. Bahia-Brazil, 2001-2015
Source: Author
The coefficient of general detection softened by the local empiric Bayesian model ranged from 0 to 270.8 cases/100.000 inhabitants. We observed that 3.6% (n=15) of the municipalities were classified as silent and 9,4% (n=39) as hyperendemic (40 or more cases/100.000), with special attention to the municipalities of An-daraí, Barreiras, Belmonte, Guaratinga, Itabela and Remanso, with coefficients higher than 100 cases/100.000 (Figure 1).
The coefficient of detection of new cases in younger than 15 years of age ranged between 0 and 127/100.000. The rate of silent municipalities was of 52.5% (n=219). Of the municipalities, 8.9% (n=37) were classified as hyperendemic (10 or more cases/100.000 inhabitants), with special attention to the municipality of Remanso, with the highest coefficient of the State (127.4/100.000), followed by the municipality of Belmonte (53.5/100.000) (Figure 1).
Of the 39 hyperendemic municipalities for the general population, 71.5% (n=28) of them were also hyperendemic for the population younger than 15 years. Of the 37 hyperendemic municipalities for the population younger than 15 years, 21.6% (n=08) were exclusively hyperendemic for this population. They are: Alcoçaba (11.7/100.000), Angical (13,3/100.000), Canavieiras (11,4/100.000), Caravelas (10,2/100.000), Ibiquera (11,7/100.000), Itagimirim (21,6/100.000), Jucuruçu (12,5/100.000) and Medeiros Neto (12,4/100.000) (Figure 1).
Regarding the coefficient of new cases with grade II physical disability, the indicator fluctuated between 0 and 4.7/100.000. the proportion of silent municipalities was of 69.1% (n=288). The highest values were seen in Glória (4.7/100.000), Jucuruçu (3.68/100.000) and Guaratinga (3.42/100.000) (Figure 1).
LISA Map demonstrated that 69.3% (n=289) of the municipalities did not show statistical significance for the coefficient of general detection, with a similar phenomenon occurring for the coefficient in younger than 15 years, with 64.7% (n=270), and for the coefficient of cases with grade II, with 58.3% (n=243). Moran Map demonstrated that 10.1% (n=42) of the municipalities were classified as Q1 in the scatter plot of Moran, according to the coefficient of general detection; 10.8% (n=45), according to the coefficient in younger than 15 years; and 7.4% (n=31), according to the coefficient of grade II disability (Figure 1).
Observing figure 1, it is possible to note that the most critical areas for the epidemiological indicators were the geographical axis from the northern region up to the west of the State, and the southern region for the coefficients of general detection and in younger than 15 years; and the northern, northeastern and southern regions for the coefficient of physical disability grade II. The municipalities of these regions were located in the quadrant Q1 (high-high) of Moran’s scatter plot, since their mean and that of their neighbors is elevated. Few municipalities were located in the quadrants Q3 and Q4, considered as transition, with six for the coefficient of general detection, two for the coefficient in younger than 15 years of age and five for the coefficient of physical disability grade II.
In table 1, we can observe the correlation of Pearson among the epidemiological and socioeconomic indicators, with statistical significance. A positive correlation was found between IMHD and the coefficients of detection in the general population and in younger than 15 years. The dimension longevity of IMHD, FIMD and FIMD “health” was only correlated to the coefficient of general detection. The index of social vulnerability (dimension work and income) was inversely correlated to the coefficient of general detection. The indexes Theil-L and Gini were correlated to the coefficients of detection in younger than 15 years and with the coefficient of grade II physical disability. The three epidemiological indicators were correlated to the IPESE indicator and its dimension “economy and finances”. Additionally, Moran’s index demonstrated that all these indicators had a spatial dependency. It is worth highlighting that all correlations were considered weak.
Statistically significant correlations between the synthetic indicators of socioeconomic, social vulnerability and income inequality performances and epidemiological indicators of Hansen’s disease. Bahia-Brazil, 2001-2015
| Indicator | Coefficient of general detection | Coefficient of detection in < 15 years | Coefficient of physical disability |
| IHMD | 0.143 | 0.113 | - |
| IHMD Renda | 0.181 | 0.117 | - |
| IHMD Longevity | 0.112 | - | - |
| ISV Work and | -0.139 | - | - |
| Income | |||
| Theil-L | - | 0.145 | 0.100 |
| Gini | - | 0.170 | 0.115 |
| FIMD | 0.127 | - | - |
| FIMD Health | 0.160 | - | - |
| IPESE | 0.227 | 0.152 | 0.101 |
| IPESE Economy and Finances | 0.236 | 0.190 | 0.133 |
Source: Author
IMHD mean was 0.594, classified as low IMHD (between 0.500 and 0.599). the municipalities with the highest IMHD were Salvador (0.759), Lauro de Freitas (0.754) and Barreiras (0.721). on the other hand, the municipalities of Itapirucu (0.486), Pilão Arcado (0.506) and Monte Santo (0.506) had the worst indexes. Regarding income inequality (Theil-L e Gini), the municipalities with the highest indexes were Maraú (0.98/0.71), Ipiaú (0.92/0.63) and Ja-guarari (0.88/0.59). the municipalities with lower inequality were Gavião (0.31/0.49), Caatiba (0.30/0.45) and Itambé (0.29/0.39).
Regarding FIMD, the municipalities Lauro de Freitas (0.747), Salvador (0.712) and Feira de Santana (0.699) had the highest values. The municipalities of Pilão Arcado (0.278), Gongogi (0.282) and Várzea do Poço (0.284) were the ones with the lowest values. The municipalities of Pojuca (0.741), São Francisco do Conde (0.748) and Madre de Deus (0.754) occupied the best ranking in IPESE. The municipalities of Pilão Arcado (0.337), Gentio do Ouro (0.378) and Buritirama (0.383) occupied the last positions.
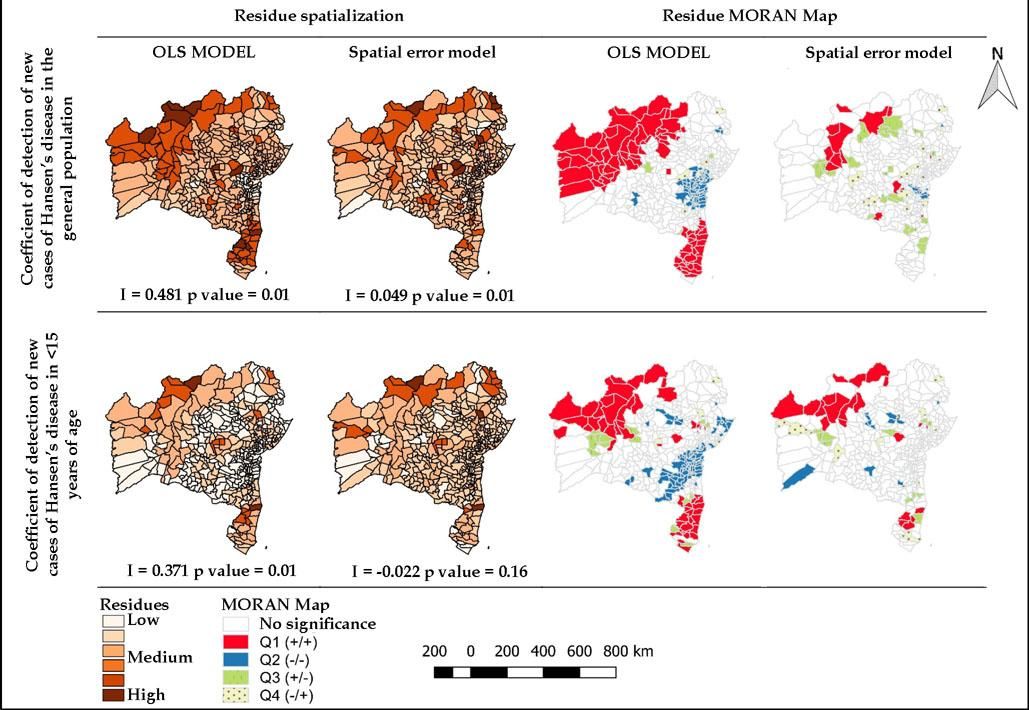
After different models through multivariate regression, only the IPESE indicator “economy and finances” had a significant coefficient of regression for two dependent variables: coefficient of detection of new cases of Hansen’s disease in the general population and in younger than 15 years. Although there was normality of residues, Moran’s statistics showed that both had spatial dependency: coefficient of general detection (Moran’s I=0.481, p=0.01) and coefficient of detection in younger than 15 years (Moran’s I=0.371, p=0.01).
The Spatial Error Model was the best indicated model by the multiplier tests of Lagrange in the robust version for the analysis of two epidemiological indicators (Robust LM-error, p<0.001). Table 2 compares the models OLS and Spatial Error for two dependent variables, having as the predicting variable IPESE “economy and finances”. In the OLS model, normality of residues was observed both for the coefficient of general detection (p=0.597) and the coefficient of detection in younger than 15 years (p=0.436) and homosce-dasticity (p=0.932 and 0.115, respectively).
Models of classic and spatial regression and comparison between models for the log of the softened coefficients of detection of Hansen’s disease in the general population and in younger than 15 years. Bahia-Brazil, 2001-2015
| Criterion | Coefficient of general detection | Coefficient of detection in the population < 15 years | ||
|---|---|---|---|---|
| OLS | Spatial Error Model | OLS | Spatial Error Model | |
| Intercept | 0.658306* | 0.60942* | 0.0321911 | 0.0456763 |
| IPESE Economy and Finances | 0.653489* | 0.648926* | 0.619965* | 0.511448* |
| R2 | 0.052706 | 0.52536 | 0.065264 | 0.436949 |
| Likelihood log | -267.072 | -142.095 | -197.772 | -109.621 |
| Akaike (AIC) | 538.145 | 288.192 | 399.544 | 223.242 |
| Schwarz (BIC) | 546.211 | 296.258 | 407.61 | 231.308 |
| Moran’s I | 0.481 | -0.049 | 0.371 | -0.022 |
Source: Author * p value <0.001
We observed that the spatial regression model improved the results, since it brought upon a better explanatory power (R2), amplification of the likelihood log and reduction of AIC and BIC. The final model was able to explain approximately 52% of the coefficient of detection of new cases of Hansen’s disease in the general population and 43% in the population younger than 15 years.
Figure 2 shows the spatial distribution of the residues of the models of classic regression and Spatial Error, as well as the Moran Map of these residues. The application of the model of spatial regression practically eliminated the spatial dependency of the coefficient of detection of new cases of Hansen’s disease in the general population (I=-0.049, p=0.009) and completely eliminated the dependency of the coefficient of detection of new cases in the population younger than 15 years (I=-0.022, p=0.16).
Finally, the municipalities were compared according to IPE-SE’s classification “economy and finances” (Table 3). Of the 417 municipalities studied, 37 of them were classified as high or very high performance (0.700 to 1.00); 50, as medium performance (0.500 to 0.699); 243, as low (0.300 to 0.499); and 87, as very low (0 to 0.299). we observed that the municipalities situated in the very high/high and medium rank had a higher burden of Hansen’s disease, with statistically significant differences when compared to the municipalities with low or very low performance.
Analysis of the epidemiological indicators of Hansen’s disease according to the level of the socioeconomic performance index- economy and finances. Bahia-Brazil, 2001-2015
| Index of socioeconomic performance - economy and finances, 2010 | ||||||
|---|---|---|---|---|---|---|
| Variable | Very high and high (1) (n= 37) | Medium (2) (n=50) | Low (3) (n=243) | Very low (4) (n=87) | Anova | Groups |
| Coefficient of general detection | 24.8±22.3 | 25.2±28.1 | 12.9±22.9 | 12.1±13.0 | p<0.001 | 1 vs (3,4) 2 vs (3,4) |
| Coefficient of detection in < 15 years | 5.27±5.7 | 5.72±9.1 | 2.46±8.8 | 2.32±4.7 | p=0.015 | 1 vs 4 |
| Coefficient of grade II physical disability | 0.64±0.7 | 0.68±1.0 | 0.24±0.6 | 0.18±0.46 | p<0.001 | 1 vs (3,4) 2 vs (3,4) |
Source: Author
The heterogeneity in the spatial distribution of Hansen’s disease in the State of Bahia resembles that of the regional and national patterns. The spatial pattern has been shown both in studies involving large areas, such as municipalities and States, and in small areas, as with the census sectors. Imbiriba et al28, in a study conducted in Manaus (AM), demonstrated, for example, that the neighboring census sectors had disparate characteristics, whereas in some distant areas had similar coefficients. In our study, the most critical areas were notably concentrated in the north-west axis and in the southern region of the State.
In these regions, a peculiar migratory pattern was observed. The south of the State, known by cocoa and cellulose production, attracted many immigrants throughout the decades in search of better quality of life. Nonetheless, in the last few years of the 20th century, with a crisis in the coca sector due to an intense loss of crops affected by the fungus Crinipellis perniciosa, there was an intense outflow of farmers towards the cities, mainly Itabuna and Ilhéus. In them, these workers occupied the peripheries and lived in precarious conditions, particularly regarding housing, education, health, nutrition and sanitation.29
In the northern region of the State, where the Vale do São Francisco is located, the installation of projects of regional development aimed at irrigated fruit farming resulted in an intense migratory flow, even considering the low salaries offered to workers.30 In 2010, for example, 35.4% of the individuals living in the municipality of Juazeiro were immigrants, corresponding to over 70.000 people that year. It is obvious that this process brought about positive aspects for the region but, on the other hand, the population growth did not correspond to the needed urban improvement, what put workers in conditions of social vulnerability due to the little or no access to minimal living conditions, such as sanitation, education and health.30
A similar process occurred in the west of Bahia. The development of agriculture, mainly because of soy plantations, the low prices of the lands and the Government incentives created opportunity for a large number of people to move from different regions of the country looking for new opportunities. As in Vale do São Francisco, in the west of the State, particularly in the municipality of Barreiras, the growth was not accompanied by urban development, prevailing socio-spatial inequalities.31
These areas of uncontrolled growth and the formation of clusters in a context of poverty, particularly at the cities surroundings, make individuals more susceptible to contamination with Mycobacterium leprae and allow for the maintenance of areas in which the epidemiological chain of transmission is kept active. These populations live in unfavorable social, economic, sanitary, housing and dietary conditions, enhancing the occurrence of the disease, contamination of children and the appearance of physical disabilities. For many authors, the migratory process that generates unfavorable socioeconomic contexts can be associated to the occurrence of Hansen’s disease.9,28,32,33
Although Hansen’s disease is associated to poor living conditions of the population, when analyzing IHMD, we found a relationship of the disease with a higher per capita income and longevity. This finding shows that the relationship between Hansen’s disease and development is not purely linear or cause-effect, where the low development is associated to higher disease burden. This assertion is based in the fact that we found a positive correlation between the indicators of human development and socioeconomic performance and the epidemiological indicators, i.e., the municipalities with the best indicators were those with the highest detection of the disease, which can have many different explanations as seen below.
IHMD is a synthetic indicator composed of three dimensions: longevity (life expectancy at birth), education (level of education of the adult population and school flow of the younger population) and income (per capita income). The dimensions “income and longevity” had a relationship with Hansen’s disease. Because it is a disease with a long incubation period, it is expected that in endemic areas the increased life expectancy increases the likelihood of the occurrence of new cases. The dimension “income” is related to access to services such as health and education, and the better access can explain the higher number of diagnoses.
Far beyond considering municipal development, it is necessary to think how it took place, since it represents a global synthesis. In the study, we observed that municipalities with the highest HDI also had the highest indexes of income inequality, being this an important topic for analysis. The relationship between inequalities (indexes of Gini and Theil-L) and Hansen’s disease was demonstrated in different studies. Freitas et al9 showed that the Brazilian municipalities with higher inequality are those with higher disease burden.
The synthetic indicator that showed a better relationship with the epidemiological indicators was IPESE and its dimension “economy and finances”, being the only variable able to compose the final explanatory model. The final model was possibly composed solely by this indicator due to the weak correlation observed in the other variables analyzed. Another factor to be mentioned is the influence of the number of units of analysis (417 municipalities).
IPESE originates from the combination of two other indexes, the index of social development and the index of economic development, and its objective is to measure the ability of the municipalities in meeting the needs of the population regarding basic services and the quality of these services. The dimension “economy and finances” takes four indicators into consideration, two of them related to the dynamics of the labor market (indexes of income of the formal worker and formal employment) and two related to the economic and financial dynamics of the municipalities (indexes of municipal product and financial independence).
The fact that the municipalities classified as very high and high performance have higher epidemiological indicators when compared to those classified as low or very low performance in IPE-SE’s “economy and finances” could be explained by the relationship between income and access to health services (index of income of the formal worker, that reflects the mean rentability of formal workers compared to Brazil’s level; and the index of formal employment, that measures the proportion of formal employment in the municipality). The increased income of individuals considerably enhances the chance of seeking a health service.34-36 Formal employment is indicated by et al37 as a determinant of the access, since according to these authors, being employed and having a contract increases the likelihood of seeking attention in these services. ISV reinforces this hypothesis since we observed an inverse relationship of this indicator with disease detection, evidencing that social vulnerability, materialized by the poor living conditions, hinders diagnosis.
The two following explanations are more specifically related to the indexes of municipal product and financial independence. While the first captures the level of gross domestic product (GDP) per capita of the municipality in comparison with the national level, the second index captures the ability of the municipality in financing its activities and offering services to the population.
The first explanation refers to the economic-financial increment in the general infrastructure of the municipalities and its impact in seeking and accessing health services by part of the population. Neri and Soares35 showed that individuals with more access to water, sanitation, garbage collection and electricity public services have higher chances of seeking health units when compared to those that do not have access to these services.
The following explanation is related to the impact of the indicators in their own local health system. As the municipalities increase their revenues, the financial amount to be compulsory invested in the health sector also increases, obeying the minimum percentage of 15%, as established in the article n. 198 of the Federal Constitution of 1988, regulated by the Complementary Law n. 141/2012. Besides the Constitution itself, the Law of Fiscal Responsibility (Complementary Law n. 101/2000) prevents the voluntary transfer of the country’s and the State’s resources to the municipalities in case of non-compliance of the application of the established minimum percentage.
After establishing health as a social right and the Sistema Único de Saúde as a way of ensuring this right, management and planning tools were developed to enhance the country’s, States’ and municipalities’ ability of investing in health actions and services. Among these tools, the Plano Plurianual (PPA), the Plano de Gestão, the Agenda de Saúde, the Plano Diretor de Regionalização (PDR), the Programação Pactuada e Integrada, the Lei de Diretrizes Orçamentárias (LDO) and the Lei Orçamentária Anual (LOA) are highlighted. These tools have an essential function to ensure the application of public resources in the strengthening of the health system.38
Initially, this scenario is capable of explaining an increase of new diagnosed cases in the municipalities for a reduction to be seen only later in the coefficients, what does not mean that people get sicker in the municipalities with better performance but only that there are more diagnoses and the under-notification in these areas is lower than in municipalities with worse economic and financial conditions. The same rationale can be applied to FIMD, the reason why a positive correlation between this indicator and the detection of Hansen’s disease in the general population was found.
The non-relationship between the dimension “health” and the epidemiological indicators can be explained by the fact that this dimension contemplates seven indexes, among which are those that are not associated to the epidemiology of Hansen’s disease, such as indexes of pre-natal consultations, the index of deaths with a defined cause, the index of vaccination coverage and the index of hospitalization for unavoidable causes. The same rationale can be applied to the dimension “education”, composed by five elements, among which none is related to the disease: index of enrollment in pre-school, index of enrollment in high school, index of quality of primary school (first years), index of enrollment in primary school and index of quality of primary school (final years).39
One limitation of this study refers to the fact that it only analysis synthetic indicators, disregarding the existing socio-spatial differences within the municipality, what could initially mask the true relationship between development and Hansen’s disease. The thorough look on this finding makes it possible to suggest that these areas have more cases diagnosed due to a higher supply and better access to services, not only health but also education, housing and sanitation, considered to be social determinants of the process of getting sick, what does not lead to the understanding that Hansen’s disease is linked to wealth standards, since its relationship with income inequality was demonstrated.
A second limitation refers to the fact that these indicators are made by the combination of diverse variables, aggregated into one index, what could make the identification and contribution of each isolated component difficult in the social determination of the disease. For example, the dimension health was nor correlated to the occurrence of Hansen’s disease but, if we analyze the ungrouped variables, we would possibly find a relationship with the Estratégia Saúde da Família (ESF) coverage, as pointed by Freitas et al.9 Therefore, we evidence the need of creating a specific explanatory model from ungrouped variables.
ConclusionsThe spatial analysis showed that Hansen’s disease has a heterogeneous distribution in the State of Bahia, concentrated in the north-west axis and in the south of the State.
The synthetic indicators analyzed revealed the complex relationship between municipal development and the process of being affected by Hansen’s disease, with a thorough analysis being needed on this topic because at the same time that we demonstrated a positive relationship between the disease and the indicators of human development, we also observed an equal relationship of Hansen’s disease with income inequality, evidencing the polysemy of this phenomenon.
More than analyzing a synthetic indicator, it is necessary to understand how the same indicator is distributed intra-locally. The most concrete explanation is that, the higher the development of the municipality, the more access the population will have to health services, having as an immediate consequence the increase in the coefficients of detection of new cases. On the other hand, the poor conditions that favor the disease itself make the diagnosis difficult.
IPESE’s “economy and finances” was the indicator with the best correlation to the disease, integrating the final model. The relationship could be explained by the improvement in the workers income and their connections to health services access, besides the effects of this outcome in the cross-sectional factors that enhance the individuals’ access (education, sanitation, access to water) and the direct effects in the investments in the health sector.
In view of the limitations of this study, we recommend that other studies are conducted using ungrouped variables, making possible the creation of an explanatory model that shows the connections of Hansen’s disease and its determinants. ❑
Financial Support: None.
Conflict of Interests: None.
