




Tinea manuum is a dermatophytosis which is often mistaken for other keratodermas, especially palmar psoriasis and chronic hand eczema. We report the use of dermoscopy as a diagnostic aid in a case of tinea manuum. The dermoscopic clue turned out to be the presence of whitish scaling located mainly in the furrows. This aspect has never been seen in other keratodermas and therefore can be considered as a useful finding to assist in the recognition of tinea manuum.
Tinea manuum (TM) is a dermatophyte infection affecting the palm and interdigital spaces, which typically presents as a diffuse white scaling/hyperkeratosis (keratoderma), with or without mild itching.1 Even though unilateral or asymmetrical involvement and concomitant infection of other sites (especially fingernails and feet) may be useful in assisting in the diagnosis of TM, its distinction from similar inflammatory dermatoses is often challenging, with consequent diagnostic delays, errors and unnecessary therapies.1 Over the last years, the applicability of dermoscopy has been extended to various “general” skin diseases, including acquired keratodermas.2-10 We report the use of dermoscopy as a diagnostic aid for a patient with TM.
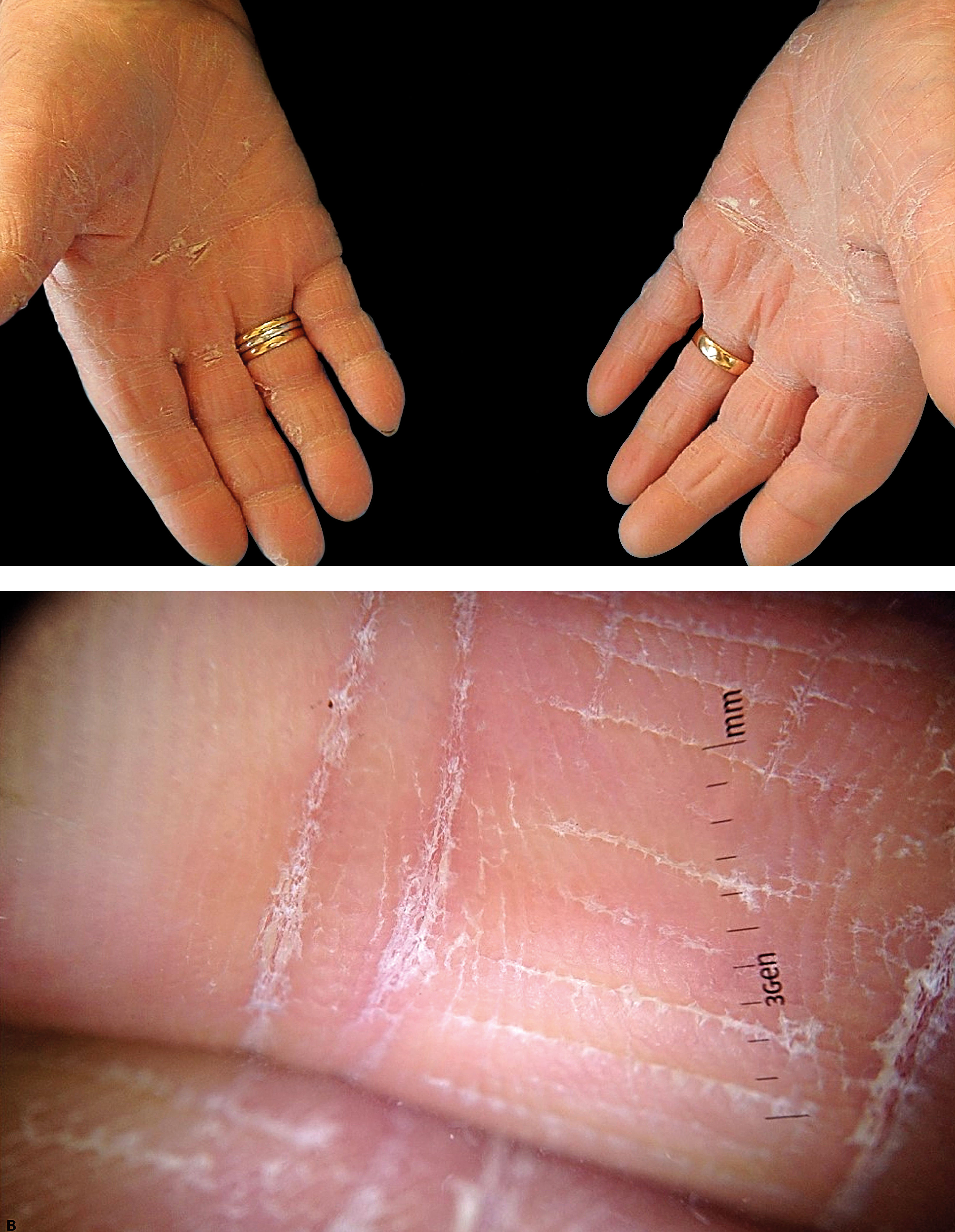
A 52-year-old Caucasian woman presented with a 3-month history of asymptomatic diffuse scaling involving the palmar surface and the volar aspect of the fingers of both hands (Figure 1A). She felt well otherwise and was not taking any medications. Her past medical history was unremarkable, but there was a family history (mother) of psoriasis. The patient had been previously diagnosed with palmar psoriasis and treated with topical steroids for about two months without significant improvement. Polarized light dermoscopic examination (carried out with DermLite DL3 x10; 3Gen, San Juan Capistrano, CA, USA) of the palms and fingers showed white scaling mainly located in the creases (Figure 1B). Direct microscopic examination of 10% KOH preparation of the scales scraped from the palmar surface showed septate branching hyphae. Cultures of specimens on conventional Sabouraud’s dextrose agar medium showed Trichophyton rubrum growth after three weeks, thus confirming the diagnosis of TM. The patient was treated with terbinafine 1% cream (twice a day) with significant improvement after four weeks.
The main differential diagnoses of TM includes palmar psoriasis and chronic hand eczema.1 Recently, we have shown how dermoscopy may be useful in assisting in the recognition of such conditions and their distinction from other relatively common acquired keratodermas, i.e. those due to pityriasis rubra pilaris and mycosis fungoides.9,10 We demonstrated that the detection of diffuse white scales is indicative of palmar psoriasis, while the presence of yellow scales, brown-orange dots or globules (corresponding to tiny spongiotic vesicles) and yellow-orange crusts is characteristic of chronic hand eczema.9 On the other hand, keratoderma resulting from pityriasis rubra pilaris and mycosis fungoides display different dermoscopic clues, namely structureless orange areas or relatively large amber scales over a white-to-pink background, respectively.10 In the present instance of TM, we found a peculiar dermoscopic finding, whitish scaling mainly located in the furrows, which has never been observed in palmar psoriasis and chronic hand eczema as well as in the other two keratodermas mentioned above. Such a characteristic arrangement of the scales is well-known in TM and it is sometimes also evident on clinical examination, especially when desquamation is marked.1 The reasons underlying this peculiar scaling pattern are not completely clear but it might result from the predilection of dermatophytes to proliferate in moist environment, such as palmar furrows.1
In conclusion, dermoscopy may be a useful tool in assisting in the diagnosis of TM by enhancing the ability to distinguish the typical arrangement of scales. Further studies on larger groups of patients are needed to confirm our observations.
Financial support: None.
Conflict of interest: None.
