








Clear cell acanthoma is an uncommon type of benign epithelial tumor. Typically, it is a solitary lesion found on the lower limbs. It presents as a nodule or small plaque with slow and well-defined growth. Diagnosis used to be clinical and histopathological, but the advent of dermoscopy has led to an increase in diagnostic accuracy. We describe a case in which dermoscopy proved highly useful for diagnosis of the lesion.
Clear cell acanthoma is a rare benign epithelial tumor with unknown etiology. It manifests clinically as a papular-nodular lesion or a small rounded erythematous plaque on the lower limbs of middle-aged adults. Women and men are affected with equal frequency, and there is no racial predilection. It is typically a solitary tumor, but there are cases with multiple lesions.
Male patient, age 64 years, reported the appearance of a nodular and erythematous lesion on the left buttock, which had occurred approximately two years previously. Dermatologic examination revealed a solitary, well-defined purple-erythematous nodular lesion, covered with discreet exudate (Figure 1).

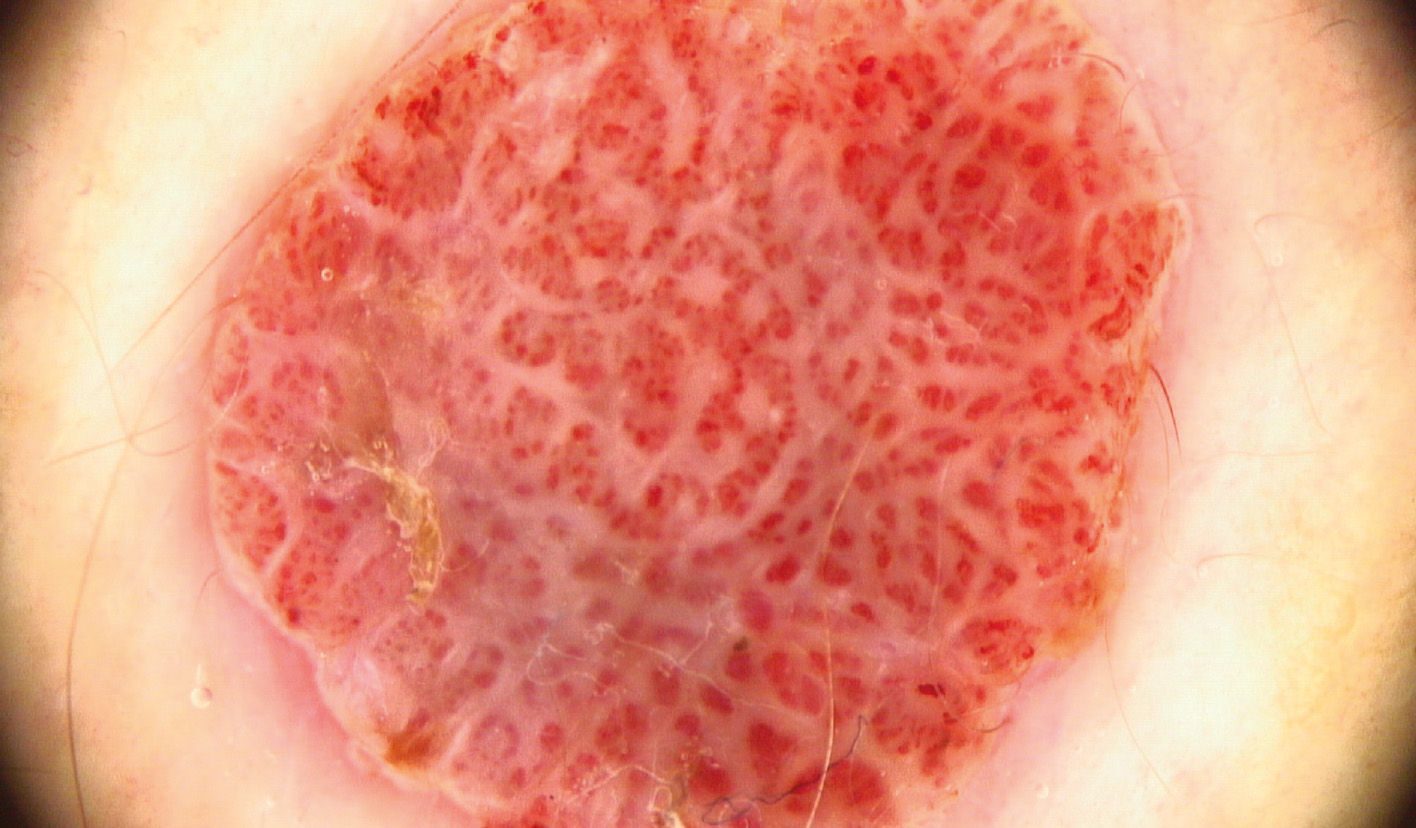
Dermoscopy showed glomerular and punctiform vessels with a “pearl necklace” distribution, an image highly characteristic of clear cell acanthoma (Figures 2 and 3).

Excisional biopsy of the lesion with histopathological examination showed dilated blood vessels in the dermal papillae and proliferation of clear keratinocytes, with sharp demarcation in relation to the normal epidermis, consistent with clear cell acanthoma (Figures 4 and 5).


Clear cell acanthoma is a rare tumor, first described by Degos in 1962.1 It presents as a slow-growing papular-nodular lesion or erythematous plaque, frequently located on the legs. The tumor is usually asymptomatic and solitary, but occasionally patients present multiple lesions.2 There may be a peripheral epidermal collarette or superimposed serous exudate. Clear cell acanthoma does not show an ethnic or gender predilection and shows a peak incidence between 50 and 60 years of age.3
Differential diagnoses include pyogenic granuloma, amelanotic melanoma, traumatized hemangioma, squamous cell carcinoma, Bowen’s disease, basal cell carcinoma, irritated seborrheic keratosis, and psoriasis.3
Dermoscopy is an excellent diagnostic test, since it shows a highly characteristic pattern. The test shows glomerular or punctiform vessels arranged in linear patterns, with a pearl necklace appearance.4 The arrangement of the blood vessels differs from that of other lesions that present punctiform and glomerular vessels. In clear cell acanthoma, the vessels are organized in a reticular array, unlike other lesions such as psoriasis (punctiform vessels distributed homogeneously in the lesion) and Bowen’s disease (glomerular vessels in clusters).5 When the lesion grows rapidly, dermoscopy may show a white peripheral Fillet, similar to that seen in pyogenic granuloma.6
Although dermoscopy is highly characteristic, histopathology is still necessary for the definitive diagnosis of clear cell acanthoma.
